傳統上,偏頭痛被認為是一種良性疼痛,長期下來是不會造成腦部和心血管功能傷害的,而隨著影像和血管檢查的發達和普遍,臨床開始發現,在偏頭痛患者發現腦白質病變(white matter hyperintensity)的機會並不稀少,研究也證實偏頭痛患者罹患腦白質病變的風險的確較高[1,2]。有趣的是,腦血管外的動脈硬化程度(arterial stiffness)也較明顯[1,3]。腦白質病變病理上的變化多半為神經髓鞘受損( loss of myelin) 和astrocytic gliosis,目前致病機轉還不確定,但多數學者認為慢性的小血管病變是可能的原因[4]。但腦白質病變在偏頭痛患者的形成原因到底是什麼? 和心血管功能有什麼相關性嗎?
流行病學
多數cohort studies與meta-analysis[2]皆證實偏頭痛患者較一般健康族群有更高的風險罹患腦白質病變。我們的本土研究中[1],利用3D CUBE FLAIR細切的核磁共振序列去偵測腦白質病變,較一般傳統FLAIR序列對於腦白質病變的偵測更為敏感和精細,發現台灣有近七成的偏頭痛患者具有腦白質病變。將白質病變作體積量化的分析,在對照控制了性別、年紀和其他血管危險因子後,發現偏頭痛患者的病變體積含量,仍大約是健康受試者的三倍之多[odds ratio = 2.75; P = 0.04]。比起健康受試者,偏頭痛患者的中央動脈血壓(central blood pressure)也較高,利用微壓計(applanation tonometry)量測脈搏波度(carotid-femoral pulse wave velocity)與動脈增幅係數(carotid augmentation index)等血管硬度指標,也發現患者的主動脈硬化程度較為明顯。
臨床的相關性
我們也發現[1],腦白質病變及動脈硬化的嚴重度和患者頭痛的臨床症狀也是息息相關。頭痛的越頻繁或程度越劇烈,腦中所測量到的白質病變量也會較多,平均的中央動脈血壓會偏高,所偵測到的動脈硬化程度也相對會越發明顯。
偏頭痛患者的主動脈硬化與腦白質病變
我們最新的研究中(圖一),除了發現腦白質病變較嚴重的患者中,主動脈的平均硬化程度較高,出乎意料地,頸動脈脈動(carotid pulsatility index, CPI)卻是下降的。由此來推測,這些患者遠端的腦內血管系統阻抗可能是較低的。
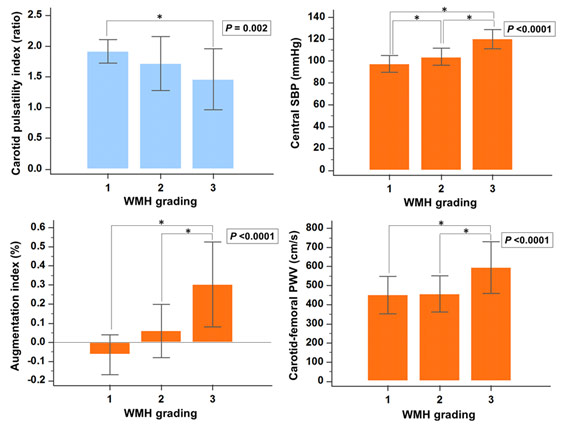
圖一: Comparisons of CPI, cSBP, AI, and cf-PWV among WMH-volume tertile subgroups of migraine patients. P values in figures were derived by one-way ANOVA followed by Scheffé’s post-hoc tests between WMH-volume tertile subgroups 1 to 3 (from lowest to highest). Error bars indicate ± one SD. *P < 0.05, pairwise comparisons. Abbreviations: CPI, carotid pulsatility index; cSBP, central systolic blood pressure; AI, augmentation index; cf-PWV, carotid-femoral pulse wave velocity; and WMH, white matter hyperintensity.
我們推測在腦白質病變較多的患者中,傷害源自於1) 硬化的中央動脈系統,因其會產生較強脈波的血流衝擊(strong central pulsatile insults),這個脈波衝擊傳遞進入腦循環系統後,如果又同時遇上2) 阻抗異常較低的腦血管系統,無法為脆弱的腦血流提供健全的設防,這二種腦心血管功能的異常合併在一起,便成為偏頭痛患者形成腦白質病變的關鍵病因(圖二)。偏頭痛患者腦部血管阻抗降低的原因目前並不清楚,但推測可能與之前科學家發現偏頭痛患者血液中具有較高濃度的血管擴張因子CGRP(calcitonin gene-related peptide)[5],以及頭痛發作時腦血管的擴張現象有關[6]。值得一提的是,在年老族群相關的腦白質病變(age-related white matter lesions)研究中,因其白質病變多為瀰漫性小血管病變(small vessels disease)引起,反而呈現與高阻抗的腦血管系統相關[7],我們研究呈現的反差結果也間接的暗示,偏頭痛患者的腦白質病變致病機轉,是與一般年老族群相關的腦白質病變致病原因不盡相同的。
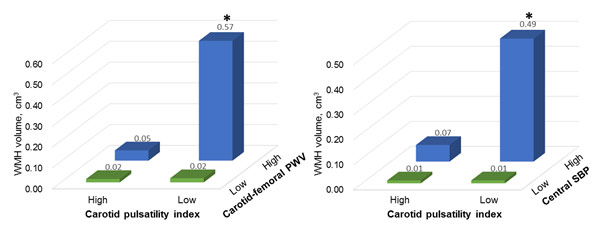
圖二: Comparisons of WMH volume between migraine patients divided by the medians of CPI, cf-PWV, and cSBP median quantiles. CPI, cf-PWV, and cSBP values were classified into low and high groups divided by median values (two quantiles for each variable). *P < 0.05 interaction effect, indicating CPI modulation of cf-PWV or cSBP effect on WMHs formation. Abbreviations: WMH, white matter hyperintensity; CPI, carotid pulsatility index; cf-PWV, carotid-femoral pulse wave velocity; and cSBP, central systolic blood pressure.
參考文獻
- Cheng CY, Cheng HM, Chen SP, et al. White matter hyperintensities in migraine: Clinical significance and central pulsatile hemodynamic correlates. Cephalalgia. 2017:333102417728751.
- Bashir A, Lipton RB, Ashina S, et al. Migraine and structural changes in the brain: a systematic review and meta-analysis. Neurology. 2013;81:1260-8.
- Schillaci G, Sarchielli P, Corbelli I, et al. Aortic stiffness and pulse wave reflection in young subjects with migraine: A case-control study. Neurology. 2010;75:960-6.
- Chung CP, Hu HH. Pathogenesis of leukoaraiosis: role of jugular venous reflux. Medical hypotheses. 2010;75:85-90.
- Bigal ME, Walter S, Rapoport AM. Calcitonin gene-related peptide (CGRP) and migraine current understanding and state of development. Headache. 2013;53:1230-44.
- Amin FM, Asghar MS, Hougaard A, et al. Magnetic resonance angiography of intracranial and extracranial arteries in patients with spontaneous migraine without aura: a cross-sectional study. The Lancet Neurology. 2013;12:454-61.
- Mitchell GF, van Buchem MA, Sigurdsson S, et al. Arterial stiffness, pressure and flow pulsatility and brain structure and function: the Age, Gene/Environment Susceptibility--Reykjavik study. Brain. 2011;134:3398-407.
- Tana C, Tafuri E, Tana M, et al. New insights into the cardiovascular risk of migraine and the role of white matter hyperintensities: is gold all that glitters? The journal of headache and pain. 2013;14:9.
對於此文章如有任何問題或指教,歡迎來信至學會,編輯部後續會將您的意見刊載在下一期會訊!